[Page 10]
Pathophysiology. The transmitral flow velocity profile is determined (like every other Doppler sampled velocity) by the instantaneous pressure difference existing between LA and the LV chambers. It begins (Figure 6b) when the LV pressure crosses (cross-over point) the LA pressure during early rapid relaxation, then accelerates in synchrony with the fall of LV below LA pressure (small but significant pressure difference), reaches its peak at the maximum atrio-ventricular pressure difference (during the suction phenomenon in the normal heart or in small LV chambers), decelerates with the reduction of the atrio-ventricular pressure difference caused by the completion of relaxation and the secondary rise in LV pressure, and the decrease of LA pressure (emptying the LA chamber), until it stops with LV and LA pressure equalization. The flow may eventually resume during diastasis (mid-diastole) even in the absence of an atrio-ventricular pressure gradient both due to inertial forces and because the LV chamber compliance is higher than the LA, a factor that favors LV filling and further LA emptying during diastasis. It is important to keep in mind that it is the relative difference in LA-LV pressure and not the absolute value of the pressures that determines the flow profile. Therefore, the same profile may be obtained in the presence of similar pressure differences but with underlying normal or high LA and LV absolute pressures.
The transmitral E wave flow profile depends in the first instance on the characteristics of LV relaxation and the relative (not absolute) position of the LA and LV pressure curves. A slowing (prolongation) of LV relaxation will reduce the local LA-LV pressure difference, reducing the peak E wave and lengthening the deceleration time, secondary to a slower rise in LV pressure (Figures 9b-d ). Conversely, a faster LV relaxation will increase the LA-LV pressure difference in early diastole (secondary to a greater reduction of LV pressure), and will therefore increase the peak E wave velocity and decrease the deceleration time (faster deceleration), in the presence of low (normal) LA pressure. Following a different mechanism, but with a similar effect on the transmitral flow profile, an isolated increase in LA pressure will increase the LA-LV pressure difference in early diastole, increasing the peak o E wave velocity. The first situation will be found in young subjects and in athletes (Figures 3-5, “normal” flow profile), the latter in heart diseases which determine an increase in LA pressure (Figures 3-5, “pseudo-normal” flow profile).
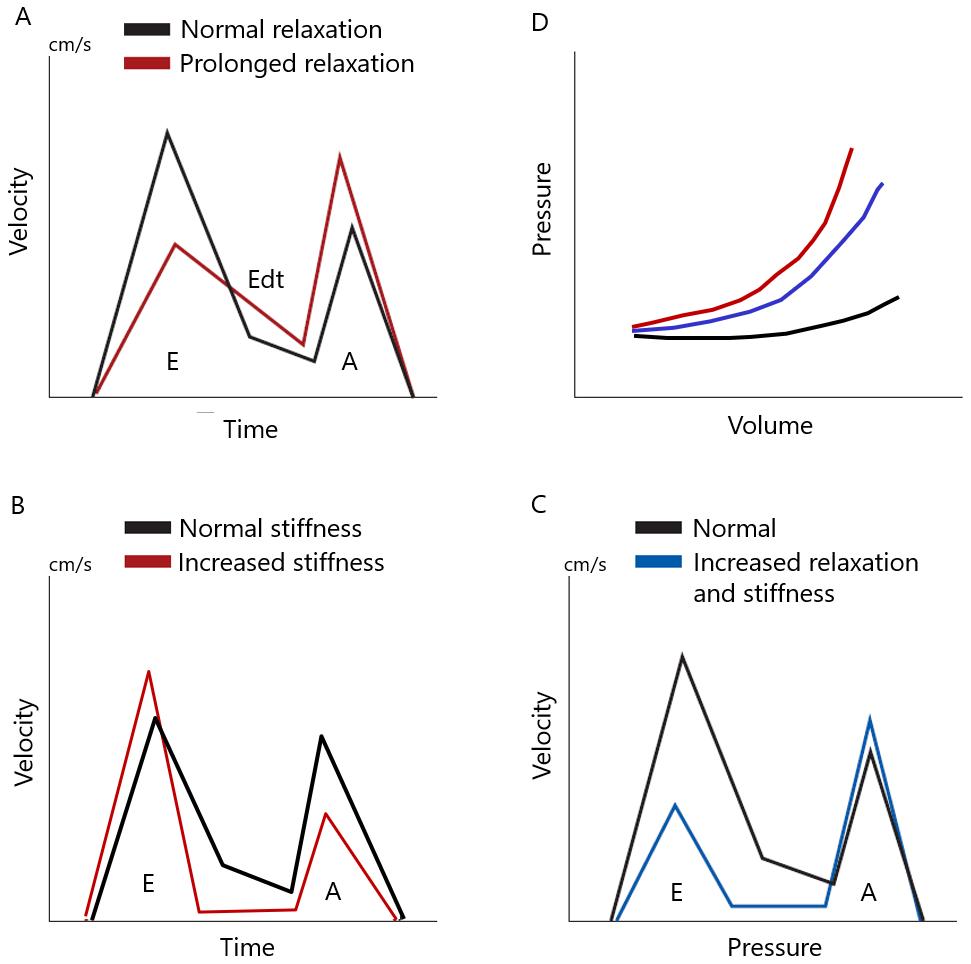
It is possible with Doppler echocardiography to differentiate the effects of a prolongation of LV relaxation from those of a reduction in chamber compliance on the transmitral flow velocity profile (8). An isolated prolongation of LV relaxation (with constant normal LV compliance) will change the transmitral profile from a normal to a profile known as “impaired/prolonged relaxation”, characterized by a redistribution of LV filling to end-diastole secondary to a reduced LV filling during early diastole; in this case the reduced early LV filling is compensated by an increase in LA systolic function (LA Starling’s law, at constant cardiac output) (Figure 2, A; Figure 3). On the other hand, an isolated reduction of LV compliance (with constant relaxation) will change the profile pattern from normal to that known as “restrictive”, characterized by a redistribution of LV filling to early diastole secondary due to an increase in filling pressures (both atrial and ventricular) necessary to overcome the increased LV stiffness, and decreased LA systolic function (and contribution to end-diastolic LV filling) secondary to increased LA afterload (i.e., LV end-diastolic pressure) (Figure 2, B and C; Figure 3). Finally, the abrupt establishment of a combination of prolonged LV relaxation and reduced chamber compliance, as during acute and prolonged ischemia (13), can result in a “mixed” flow profile, characterized by a reduction in the peak velocity and duration of the E wave, a reduction of deceleration time, and unchanged A wave (Figure 2, C and D). In this situation, the significant reduction in early-diastolic filling (secondary to marked prolongation of relaxation and increase in LV early diastolic pressure) is not adequately compensated for by an increase in the LA contribution to LV filling in end diastole, secondary to the mechanism known as LA afterload mismatch. The result will be a reduction in cardiac output.