[Page 17]
DYNAMIC MANEUVERS
Carotid sinus massage. A heart rate> 90 bpm can cause “fusion” of the transmitral flow and annular tissue Doppler waves, and the resulting fused waves cannot be analyzed. A carotid sinus massage produces a negative chronotropic effect on the heart and vasodepressive effects on arterial resistance. The negative chronotropic effect lengthens the diastolic filling time, and separates the partially or completely fused waves (due to high heart rate) (Figure 17).
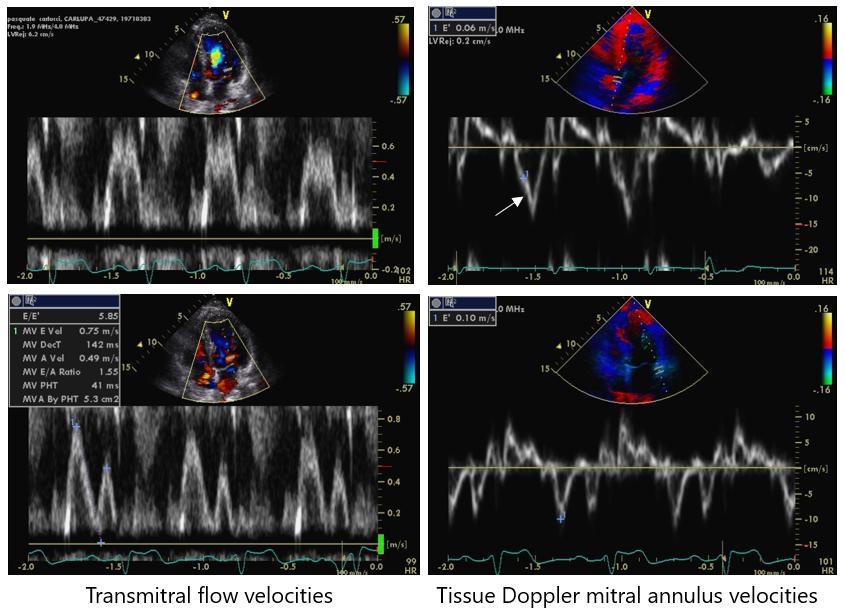
Figure 17. Carotid sinus massage. A heart rate >90 bpm (upper panels) can cause a “fusion” of the early and late diastolic transmitral peak E and A waves or of the mitral annulus tissue Doppler e’ and a’ peak waves, which may be impossible to analyse. A carotid sinus massage (lower panels) produces a negative chronotropic effect at the cardiac level, and a vasodepressive effect at the level of systemic arterial resistances. The former prolongs the diastolic filling time and separates the partial or completely fused waves.
Figure 18. Valsalva maneuver. The Valsalva maneuver produces in the early phase II an increase in intrathoracic pressure such as to significantly reduce systemic venous return and LV preload. However, the reduction in venous return can vary greatly from patient to patient. In the phase II of the maneuver, when stable and of such duration as to allow echocardiographic evaluations, the reduction in venous return produces a drop in cardiac output and reflex tachycardia. At the end of the maneuver, in the “rebound” phases III-IV, the normal negative intrathoracic pressure is restored with rapid filling of the pulmonary vascular bed (phase III), hypertension and reflex bradycardia (phase IV) secondary to the re-establishment of venous return and cardiac output, in the presence of continued sympathetic stimulation and arterial vasoconstriction. The response of the transmitral flow profile to this preload manipulation is useful for the estimation of LV FP: if the latter are normal, a proportional reduction in mitral E and A waves is observed; if the LV FP are high, there is a prevalent reduction of the E wave and associated reduction ≥0.5 in the E/A ratio (Figure 19). This index has a high specificity for detecting increased LV FP.
Diastolic stress test. Many patients with LV DD have symptoms, especially during exertion, due to the increase in the LV FP necessary to maintain an adequate LV preload for stroke volume. Therefore, it is useful to evaluate LV filling also during exercise (on the semi-supine cycloergometer). The measured parameters are: E/e ‘, isovolumic relaxation time and pulmonary systolic pressure (estimated by continuous Doppler examination of tricuspid regurgitation).