Introduction to the Methodology
Introduction to the methodology of transthoracic echocardiography: requirements and technical considerations
April 10, 2022
(updated April 16, 2022)
Pages 1 – 8
[Page 1]
Table of Contents
- Why the echocardiogram
– Orientation & nomenclature - Requirements
– Education - Time requirements
– Efficay vs. efficiency - Technical considerations
– Patient position
– Ergonomics
– ECG tracing
– Respiratory tracing
– Respiration control
– Variability in echocardiography - Information provided by the method
- Conclusions
[page links at the bottom of the page]
Today different imaging techniques are available (echocardiography, angiography, computed tomography, magnetic resonance imaging, radionuclides). The choice is based on:
- Local expertize
- Availability
- Costs
- Patient preferences
So why choose an echocardiogram ?
Circulation 1997;95:1-79
- Minimum discomfort for patient & no risks
- Unique noninvasive informations
- No iodizing radiations (contrast)
- Portability
- Immediate availability
- Repeatability
- But best used after accurate history taking, physical examination, ECG, chest X-ray, to formulate a precise diagnostic query
Which knowledge is required to learn echocardiography ?
- Knowledge of the echocardiographic machines, of ultrasound physics, and of the rationale underlying utilization of both in cardiology
- Mastering of the echocardiographic scanning techniques
- In depth knowledge of the anatomy of the cardiac fossa and of cardiac physiopathology
Orientation & nomenclature – 定向及命名法
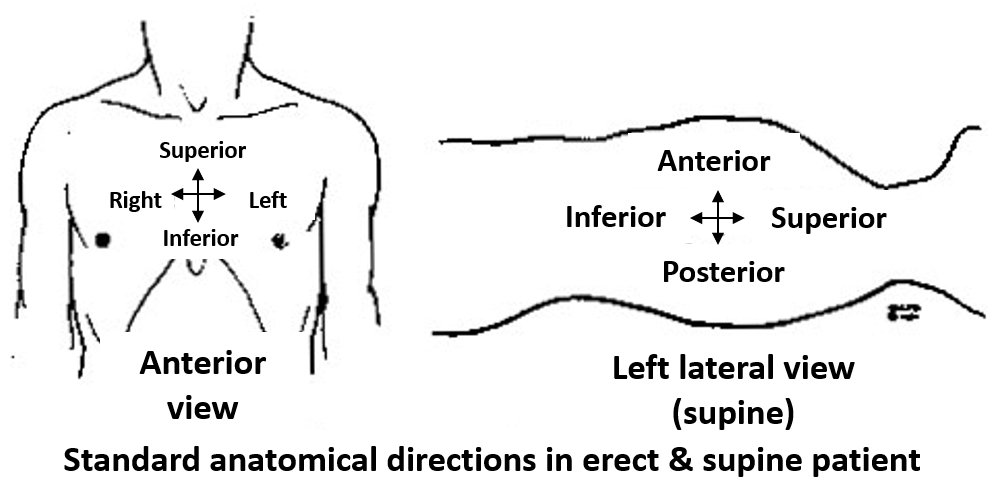
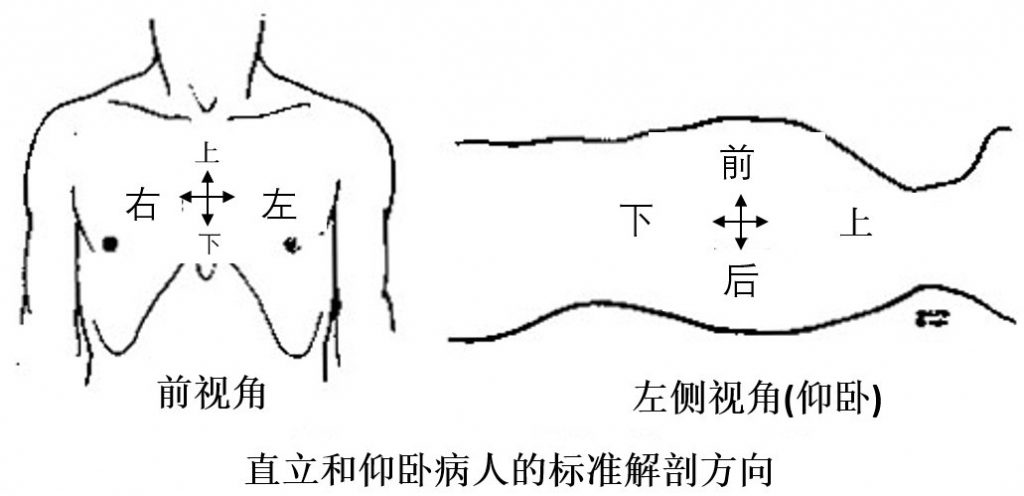
Nomenclature is very important to be able to localize unequivocally any imaged anatomical structure within the cardiac fossa and more generally in the thoracic cavity. Nomenclature should be shared with neighboring professional figures (surgeons, invasive cardiologists, electrophysiologists).
An example, the left atrium:
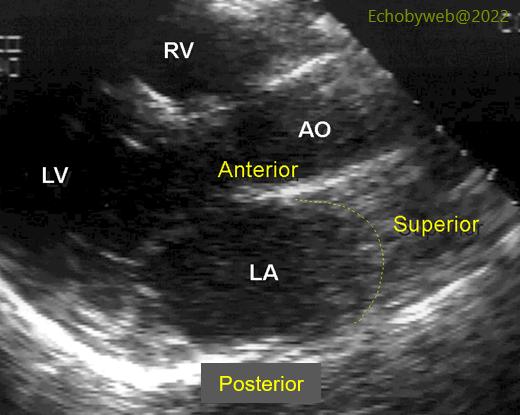
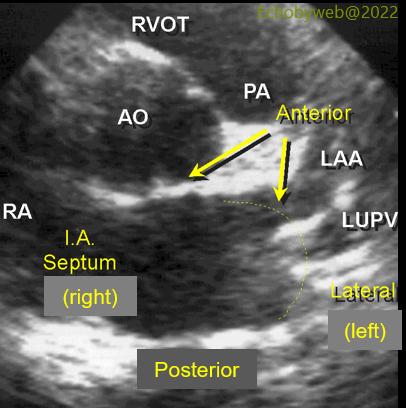
Figure 1. The LA walls as seen in a parasternal long axis view (refer also to Figure 1). The anterior wall aligned with the aortic root is antero-medial. The posterior wall faces the spine. The pulmonary veins enter the LA between the posterior and superior walls. Figure 3. Antero-medial (below the aortic root) and antero-lateral (with the LA appendage orifice, LAA) LA walls. The interatrial septum is medial (right). The left upper pulmonary vein (LUPV) is seen below the LAA.
RVOT: RV outflow tract.