[Page 2]
Requirements.
“Echocardiography is extremely operator dependent and its optimal performance requires an operator with adequate education and high technical skills, which is able to continuously integrate:
– known clinical information,
– information included in ultrasound imaging,
– and the physio-pathological data
to adequately address the examination such that it is complete and accurate.”
(J Am Soc Echocardiogr 1992;5:635)
For example:
Education may have dramatic influence on accuracy and perceived “clinical outcome”
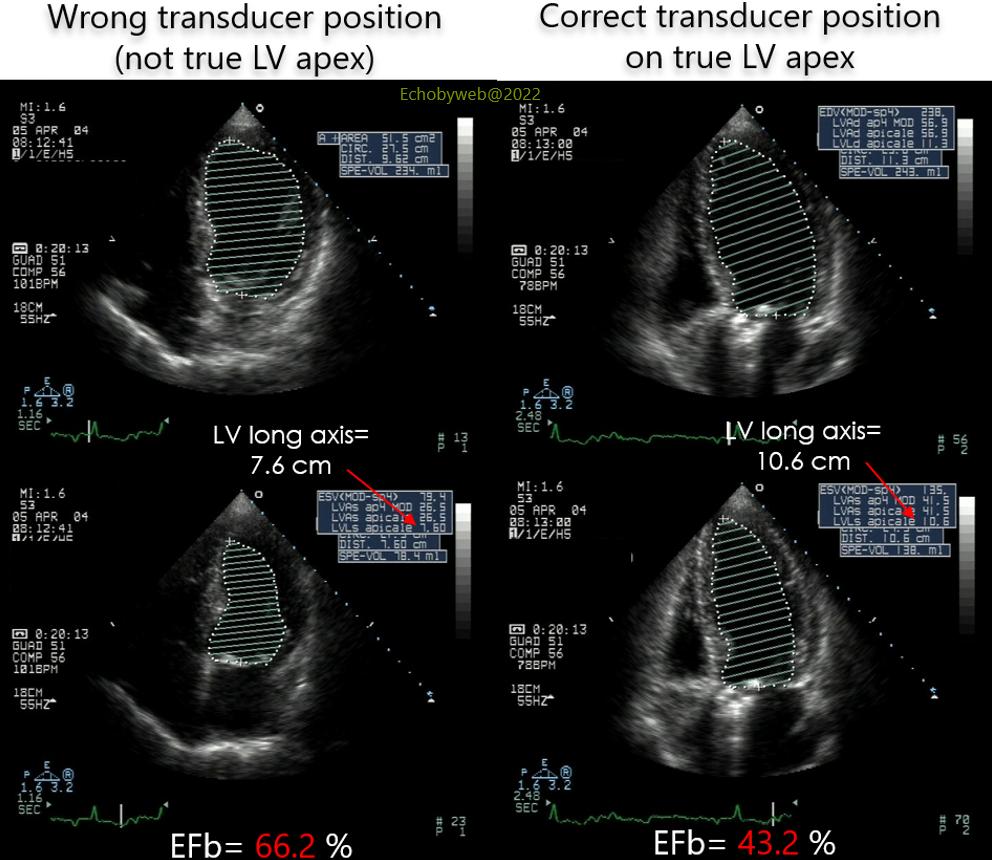
Figure 4. Follow-up exam after aortic valve replacement (mechanical prosthesis). In this “real-life” example, the erroneous positioning of the ultrasound transducer below the left nipple, instead of the true LV apex, leads to a significant underestimation of LV volumes (especially the end-systolic), which translates into a dramatic overestimation of LV ejection fraction. In this example, the operator (a cardiologist) had a long-standing experience as an echocardiographer, but evidently an inadequate original training. Being considered “elder” staff, no fellow-in-training (and as such aware of the problem) dared to suggest a correction. After 2 years of outpatient follow-up, the error was finally detected and ACE-inhibitor therapy initiated, which led to near normalization of EF after 6 months.
Echocardiographic imaging should only be performed by laboratories with adequately trained medical and technical staff which complies with the recommendations concerning the number of performed exams described in the ACC/AHA Recommendations (Circulation 1997;95:1686)
Complete examination
The echocardiographic examination should be complete (including 2D, M-mode, Doppler echo, color Doppler, tissue Doppler modalities) using all available ultrasound views.
Focused examination
The echocardiogram is performed with the aim to – and limiting it to – answer a specific diagnostic query.