[Page 5]
PHYSIOPATHOLOGY
Optimal LV performance depends on its ability to cyclically switch between 2 different states:
1) a compliant chamber in diastole which allows LV filling with low FP;
2) a stiff chamber in systole (steep rise in LV pressure) with ejection of the systolic volume at (high) arterial pressure values.
In a normal situation, the LV DF allows the ventricle to reach through diastolic filling a preload (which is not the end-diastolic pressure, but the degree of stretching of the muscle fiber cells at the beginning of the systolic contraction) which is adequate to obtain, through the interaction with the contractility (positive relationship) and LV afterload (negative relationship), a normal systolic stroke volume, avoiding an increase in FP. As mentioned, it is not possible to discuss separately systolic and diastolic function: both influence each other and in the contraction-relaxation cycle they can be considered the 2 sides of the same coin, because contractility and relaxation share the same mechanisms and determinants. A pathogenic noxa that impairs contractility will also alter relaxation, and vice versa. The diagram in Figure 1 exemplifies how stroke volume results from both functions. Today, the pathophysiology of various cardiac diseases is interpreted as a combination of the impairment of both systolic and diastolic functions, or even as a prevalent alteration of the latter (ex,: hypertrophic cardiomyopathy; “restrictive” cardiomyopathies; hypertensive heart disease).
It should be noted that, while on the one hand the mechanical systolic function (measured as ejection fraction) recognizes contractility as the main determinant, LV DF recognizes two main determinants: relaxation and chamber compliance (or its reciprocal, stiffness). The definition “DD” is thus relatively imprecise, as it can refer to an isolated alteration of relaxation (which occurs in the early stages of many cardiac diseases, and corresponds to grade I of DD), to prevalent alteration of LV chamber compliance (ex: restrictive cardiomyopathy), or to an impairment of both relaxation and chamber compliance (grades II and III of DD (Figures 4 and 5). For example, we can consider both ischemic heart disease with preserved ventricular geometry and LV hypertrophy as examples of prevalently impaired ventricular relaxation, while advanced dilated cardiomyopathy (primary or ischemic) as an example of combined impairment of LV relaxation (prolonged) and chamber compliance (reduced). In the clinical setting, changes in relaxation and chamber compliance recognize different causes: LV hypertrophy, an increase in LV afterload and acute myocardial ischemia cause a prolongation of myocardial relaxation (which is energy-dependent), whereas LV myocardial fibrosis (if sufficiently extended) can reduce chamber compliance.
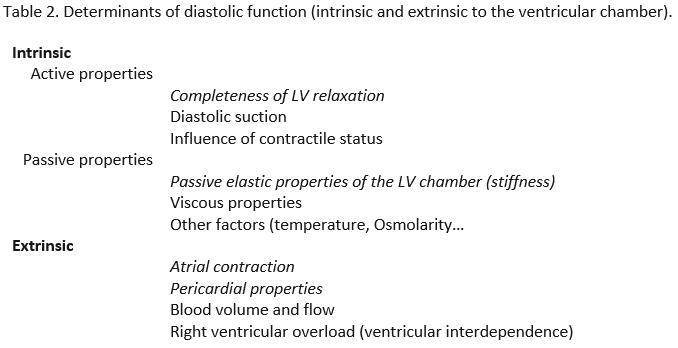
Determinants of diastole.
Table 2 shows an exhaustive list of the determinants of LV DF, divided between intrinsic and extrinsic, the most important in italics. The main difference between LV relaxation and LV chamber compliance (the LV passive elastic properties) is that the former is a rapid, energy-dependent process, while the latter is passive and slower, and is related to the trend of LV pressure and volume increase between mid and end-diastole.