[Page 9]
Transmitral flow profile. The transmitral flow profile is used to estimate both LV relaxation and chamber compliance. However, since all the above factors can influence these estimates, our deductive reasoning must take them into account.
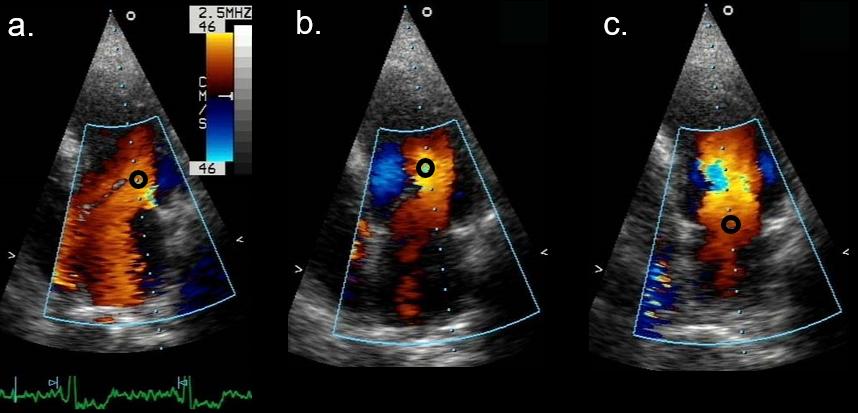
Sampling methodology. The sample volume (2-3 mm) must be positioned between the apex of the mitral leaflets in diastole, in the 4-chamber apical view, always guided by color Doppler imaging, to correctly position the sample volume at the point of maximum acceleration of flow. Since we are using pulsed Doppler, we must first detect with color Doppler the location of maximum flow velocity (Figure 9a). A sample volume positioned too distal in the LV cavity (relative to the mitral leaflets) or too proximal in the LA may under/overestimate early and end-diastolic peak velocities, and artifactually modify the flow velocity profile (and its interpretation) with non-standard measures (Figure 9b and 9c). It is equally important to align the sample scan line with the direction of flow (to make the most of the “Doppler shift” phenomenon). Since the direction of flow constantly deviates towards the LV lateral wall with LV dilation and systolic dysfunction, the transducer must be moved away from the apex, towards the lateral wall (on the chest: towards the patient’s left armpit).
Figure 9a. Color Doppler (normal) transmitral flow, apical 4-chamber view.
Figure 9b. Different positioning of the pulsed Doppler sample volume:
a. correct position between mitral leaflets where maximum flow velocity (color Doppler) is seen. Measurements are standard.
b. sample volume position too distal in LV cavity.
c: sample volume position too proximal in LA cavity.
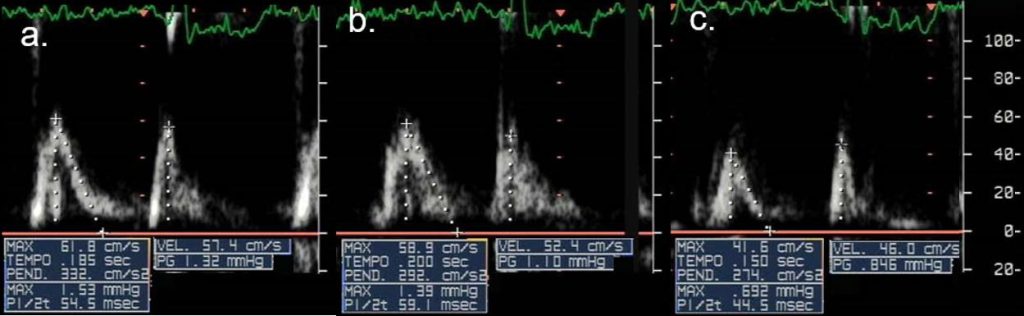
Figure 9c. Measurements at corresponding sampling position (Figure 9b).
a: standard measurements (max: peak velocity; TEMPO: E wave deceleration time.
b: lower peak E velocity, longer E deceleration time.
c: lower peak E velocity, shorter E deceleration time.
Measurements. On the transmitral flow velocity profile we measure (abnormal cutoff values are shown in Table 3): 1) the E and A wave peak velocities (Ep, Ap) (Figure 9d);
2) the E/A ratio;
3) the E wave deceleration time Edt (extrapolated to the baseline velocity= 0);
4) the A wave duration (Adur).
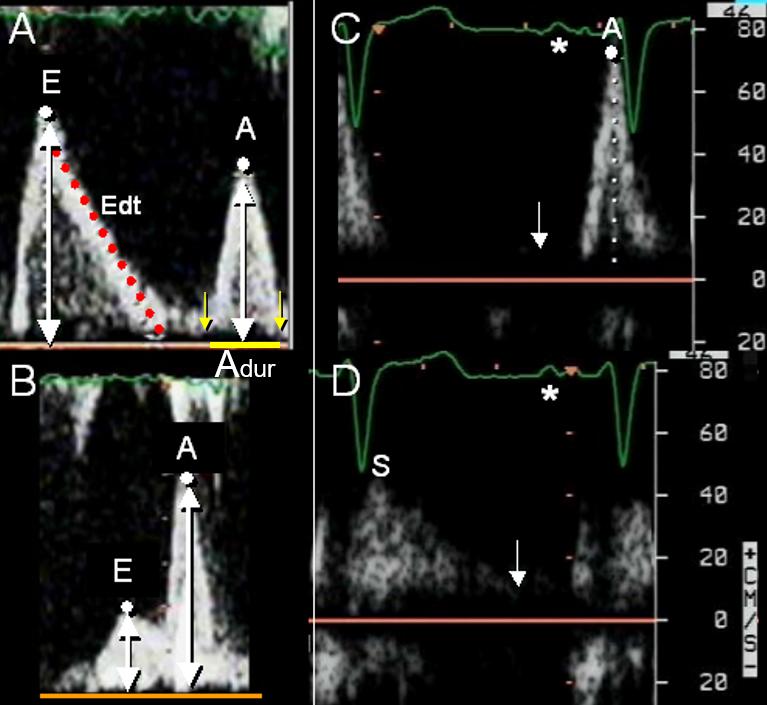
Figure 9d. Measurement of the transmitral flow profile.
A. Normal flow velocity profile. A: peak A velocity; E: peak E wave velocity; Edt: E wave deceleration time (red dotted line, from peak E to the zero velocity baseline).
B. Markedly prolonged relaxation flow velocity profile. Note the very low peak E wave velocity. Also, E deceleration time cannot be measured because of the partial fusion of the E and A waves. The asterisk marks the ECG P wave: the presence of the ECG is important in that it allows a clear distinction between the early diastolic E and the late diastolic A waves.
D. As in B, but with pulmonary venous flow velocity profile: no early diastolic D wave is detectable.
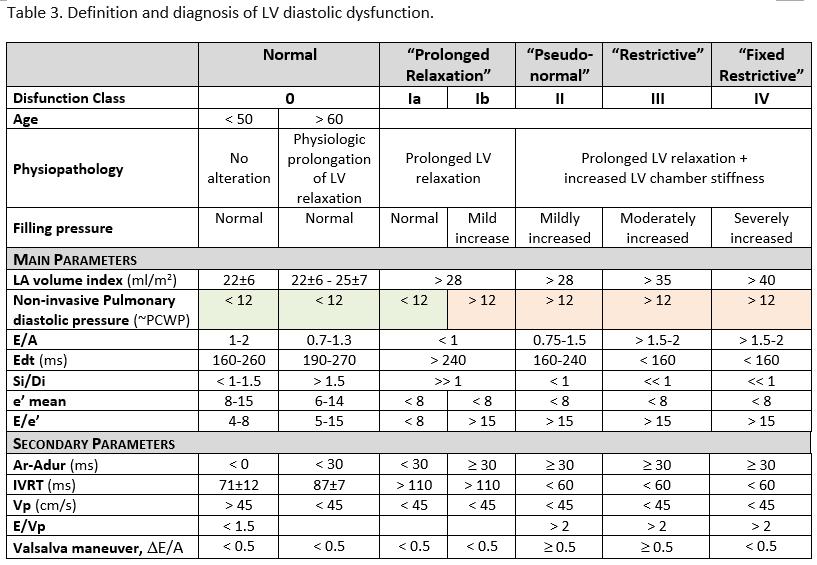
Table 3. Notes:– It is necessary to evaluate in the individual patient the influence of heart rate and preload (hypovolemia; mitral valve regurgitation; stroke volume) and to integrate the clinical picture (presence or absence of shortness of breath) and the standard echocardiographic data (ex: LV hypertrophy; grade of mitral regurgitation…).
– The Class I DD (Prolonged Relaxation) is subdivided here into two sub-classes: Ia and Ib, characterized respectively by normal and mildly increased LV filling pressures. The subdivision is obtained using non-invasive pulmonary diastolic pressure.
– Non-invasive pulmonary diastolic pressure: obtained by CW Doppler sampling of PR with the following formula= end-diastolic gradient + estimate of RAP (using IVC inspiratory collapsibility).
– E/e’ parameter: in the presence of LV diastolic dysfunction Ia and Ib, the values between 8 and 15 are indeterminate; it is necessary to integrate with other indices.
– Ar-Adur: time difference between the duration of the anterograde (transmitraL flow) and the retrograde (pulmonary venous flow) A wave
CW: continuous wave; e’: tissue Doppler mitral annulus early diastolic wave; Edt= transmitral E wave deceleration time; E/A: transmitraL peak e And A wave ratio; IVC: inferior vena cava; IVRT: isovolumic relaxation time; LA: left atrial; LV: left ventricular; PCWP: pulmonary capillary wedge pressure; PR: pulmonary regurgitation; RAP: right atrial pressure; Si/Di: systolic/diastolic ratio of the pulmonary venous flow velocity-time integrals; Vp: color M-mode mitral flow propagation velocity