[Page 13]
Pericardial constriction, pulsed Doppler examination.
Figure 86A. Note the 59% increase (from 61 to 97 cm/s) in mitral peak E wave at the first expiratory beat.
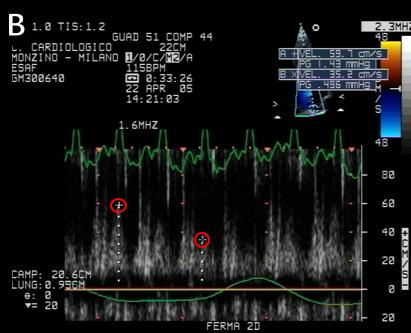
Figure 86B. Note the 34% decrease of the LV outflow peak velocity (from 94 to 62 cm/s) during inspiration.
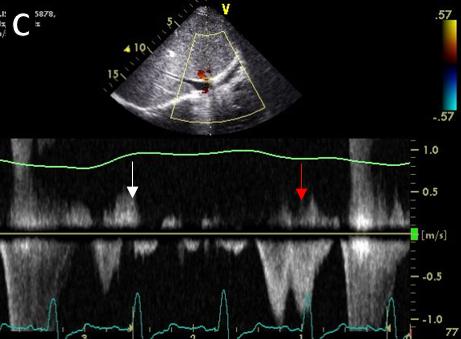
Figure 86C. Tissue Doppler velocities of the lateral mitral annulus: a respiratory change in e’ can be seen.
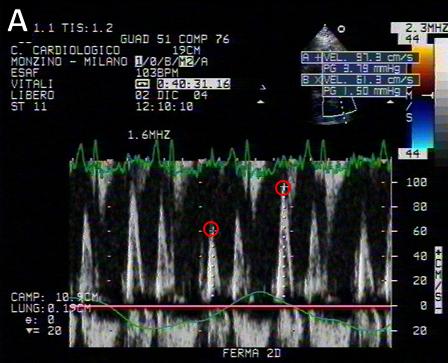
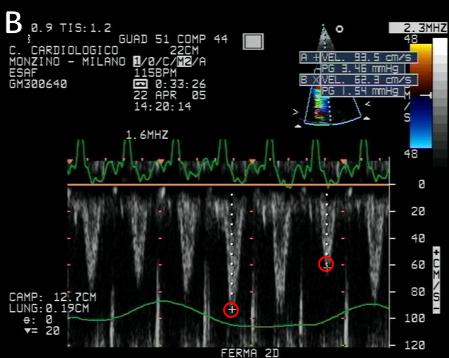
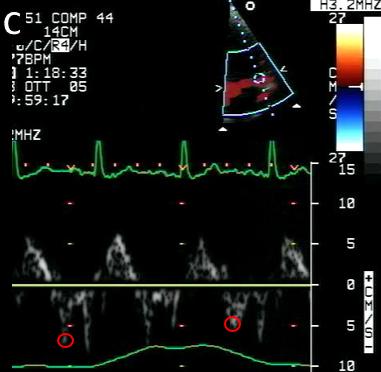
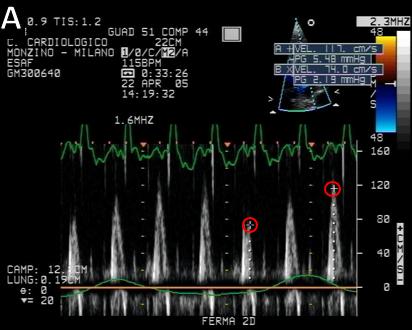
Figure 87A. Note the 58% increase (from 74 to 117 cm/s) in mitral peak E wave at the first expiratory beat.
Figure 87B. Note the 71% increase of the forward diastolic pulmonary vein peak velocity (from 35 to 60 cm/s).
Figure 87C. Pulsed Doppler hepatic vein flow velocities: there are marked respiratory changes in right atrial inflow velocities with an increase during inspiration and decrease / reversal during expiration.
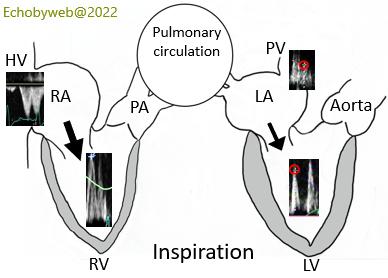
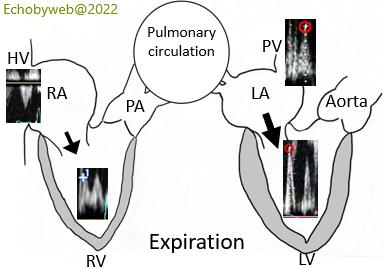
Figures 88-89. Right and left heart reciprocal modifications of filling velocities during respiration. During inspiration there is an increase in RA and RV inflow with reciprocal reduction of LA and LV inflow. During expiration, the increased gradient between pulmonary capillary wedge pressure and LV diastolic pressures causes an abrupt increase in mitral peak E velocity (see also Figure 81).
Epidemiology of pericardial constriction.
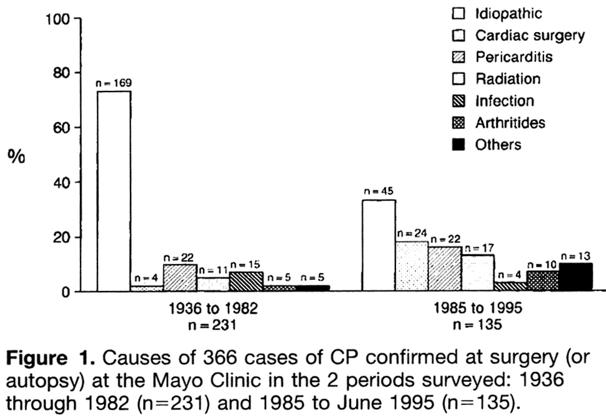
Figure 90.
Ling LH et al. Constrictive pericarditis in the modern era. Evolving clinical spectrum and impact on outcome after pericardiectomy (Circulation 1999;100:1380-6)