[Page 4]
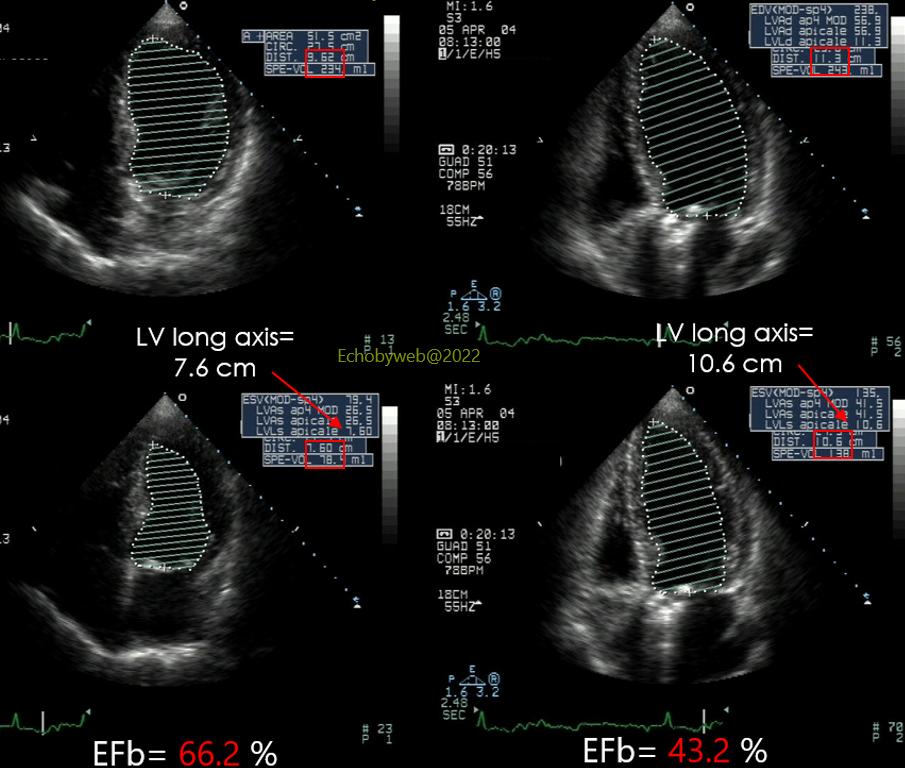
Figure 9. An example of the consequences of LV foreshortening.
In this patient, foreshortening is prevalent in systole, the LV long axis is foreshortened from 10.6 cm (right panel) to 7.6 cm (left panel), which produces a great overestimation of EF= 66.2 % (overestimated) vs 43.2 % (correct value).
The clinical consequence of this incorrect evaluation was that the patient was withheld from ACE-inhibitors for 2 years.


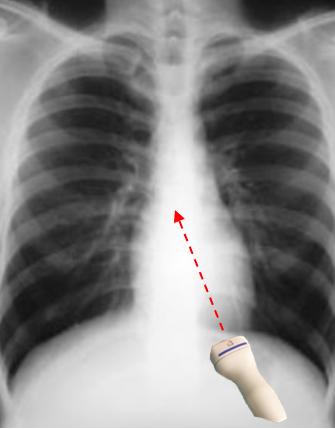
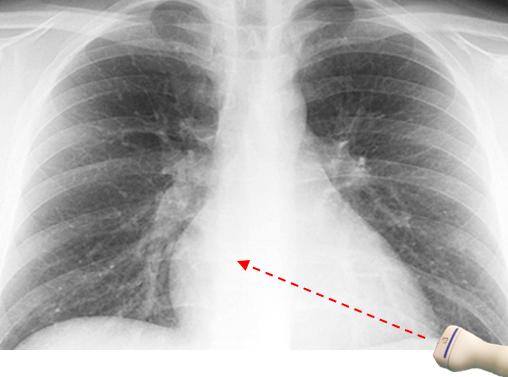
The correct transducer position to obtain the true LV long axis in the 4-chamber view is very often much more lateral than initially imagined by the operator. Figure 11 shows the correct position of the transducer along the mid-axillary line, whereas in Figure 10 the transducer is erroneously placed anterior to the anterior axillary line. The position of the transducer depends obviously on the alignment of the heart within the thorax: when the heart is positioned vertically (Figure 12), then the correct transducer position is similar to that shown in Figure 10. In contrast, when the heart is more horizontal (Figure 13), the correct transducer position is at the mid or posterior axillary line (Figure 11).