[Page 3]
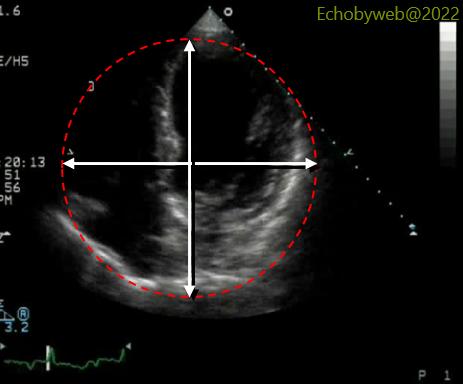
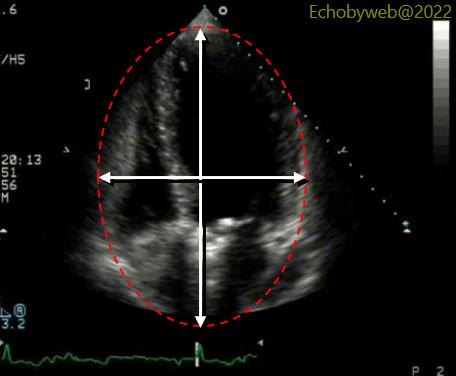
The result of an incorrect transducer position on the anterior apex, instead of the true apex, is that the cardiac fossa (the whole cardiac area) appears as a circle (Figure 5) instead of what it is in reality (even in dilated cardiomyopathy with a spherical LV): an oval (Figure 6).

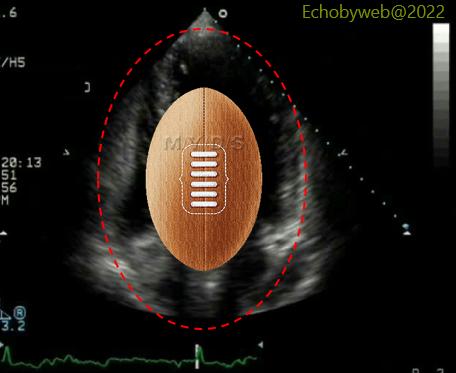
The cardiac fossa should resemble a rugby ball and not a football. This method should be used to quickly separate an acceptable imaging from an image that should be discarded. This method can be easily applied to any echocardiographic examination to decide if it can be accepted or rejected based on image quality: if the operator (sonographer or cardiologist) has acquired imaging with an erroneous transducer position, this jeopardizes the whole exam because it means that the operator is not aware of the problem (which is a basic skill), unless it is stated in the report that there was no other way to obtain a 4-chamber view. Of note, LV volumes and EF should not be measured in this setting.