[Page 3]
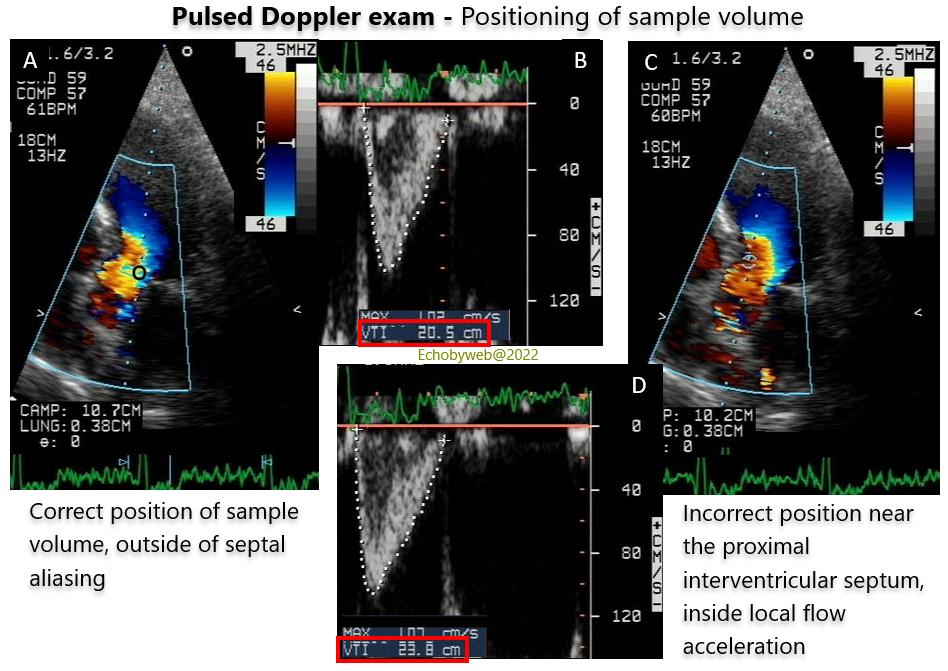
As shown in Figure 9, the pulsed Doppler sample volume should be preferentially positioned on the side of the mitral valve annulus (Figure 9 A-B), so to avoid the local acceleration that is usually near a mild proximal interventricular septal hypertrophy, which is quite common in some populations (Figure 9 C-D).
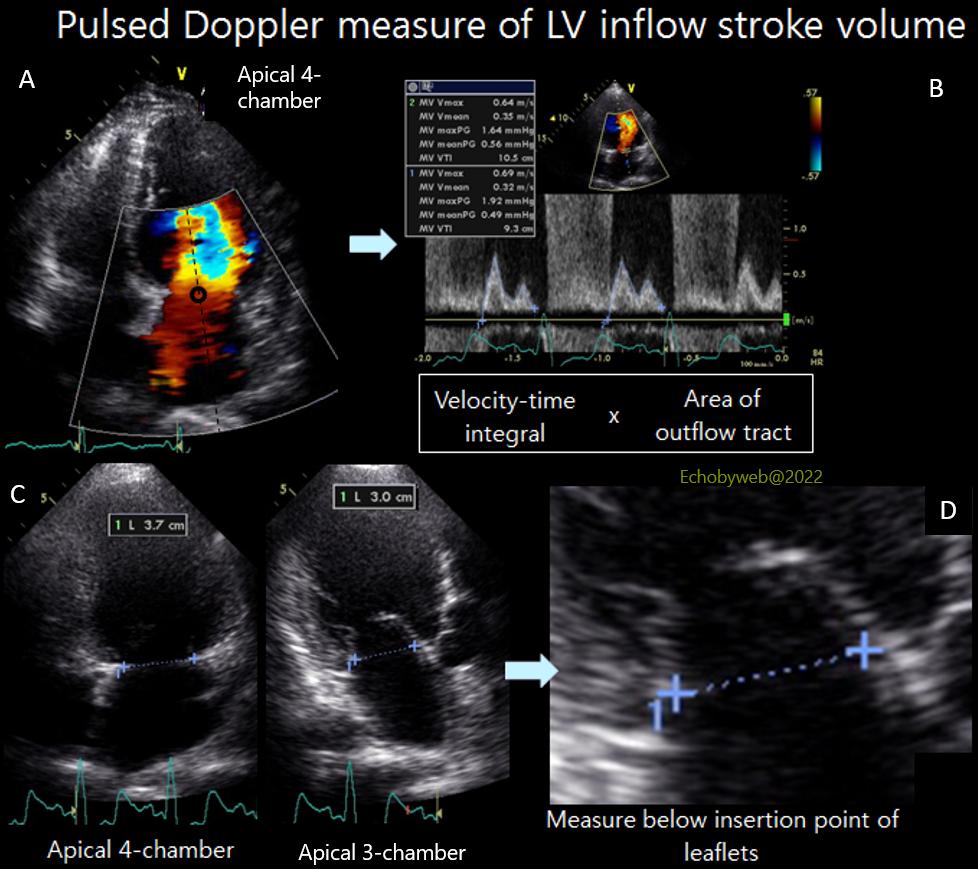
In the absence of more than trace mitral regurgitation, LV stroke volume can also be calculated from LV inflow at the mitral valve annulus level, following these suggestions:
– The sample volume should be positioned centrally at the level of the mitral valve annulus in diastole (learning curve required) (Figure 10, A).
– It is acceptable to consider the area of the annulus fixed during diastole.
– The planimetry of the velocity-time integral should be performed excluding the eventual spectral velocities found in diastasis (personal data of the Author) (Figure 10, B).
– The measurement of the mitral annulus should consider the annulus as an ellipse, thus applying this formula to calculate the area= π x (inter-commissural diameter / 2) x (antero-posterior diameter / 2)
(you can calculate the mitral valve area here in this website); the intercommissural diameter is the longest diameter measured between the apical 4-chamber and 2-chamber views, whereas the antero-posterior diameter is that measured in the 3-chamber view (Figure 10, C-D).
Differently from the aortic valve annulus, the mitral valve is generally an ellipse, which may become circular in patients with mitral valve prolapse, or dilated cardiomyopathy. However, the assumption (simplification) of a circular mitral annulus leads necessarily to a significant overestimation of the mitral valve stroke volume in the majority of patients – and thus of mitral regurgitant volume and EROA (see Quantificatification of Mitral Regurgitation and the Calculator to estimate mitral regurgitation). Unfortunately, the present Guidelines and most published papers use the assumption of a circular mitral annulus, jeopardizing measurements and leading to overestimation of the severity of mitral regurgitation.