[Page 5]
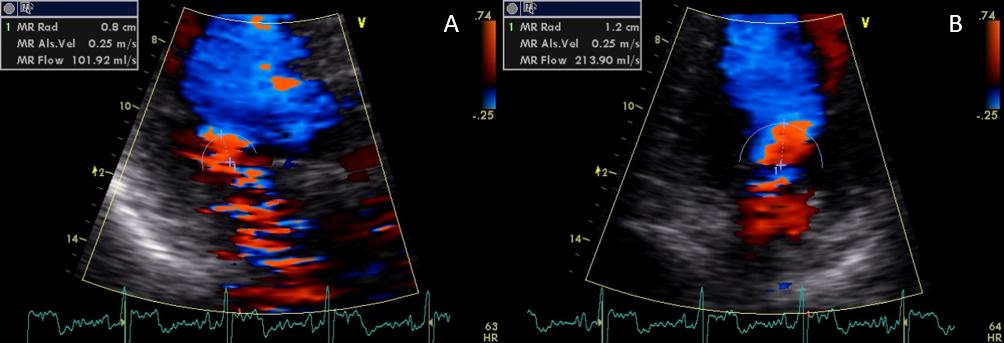
Now let’s move to the apical 3-chamber view, switch on color Doppler (Figure 11), move downwards the aliasing velocity limit to 25 cm/s (Figure 13) and search for the widest mitral flow convergence hemi-area, which we find in the 4-chamber view (compare B to A in Figure 13). If we average the PISA quantitative evaluation: made in the 3-chamber and 4-chamber views we obtain: EROA= 0.27 cm2; regurgitant colume= 28 ml; regurgitant fraction= 29%. This assessment points to an almost moderate grade of regurgitation.
So, at this point, we would have ischemic heart disease with a secondary mitral regurgitation grade 3 and normal left atrial pressure.
However, the PISA method has a number of assumptions, one of these is that the regurgitation is assumed to be holo-systolic. If the duration is less than that, then the PISA method overestimates the regurgitation grade. We have seen on Page 4 with color M-mode that the regurgitation in this patient is limited to the first half of systole.
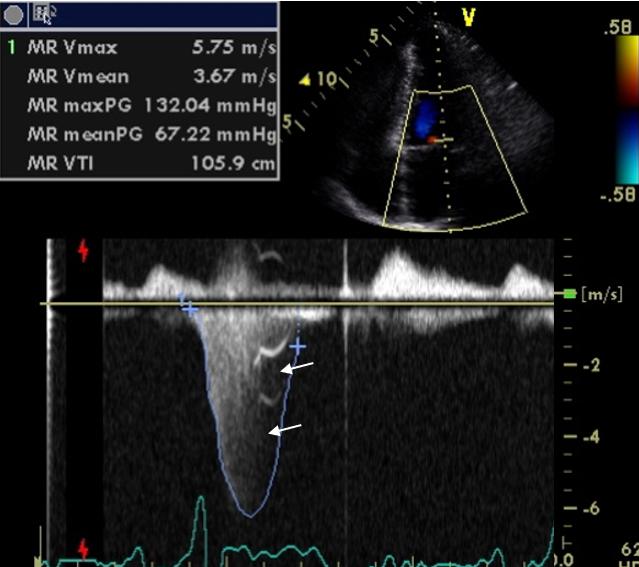
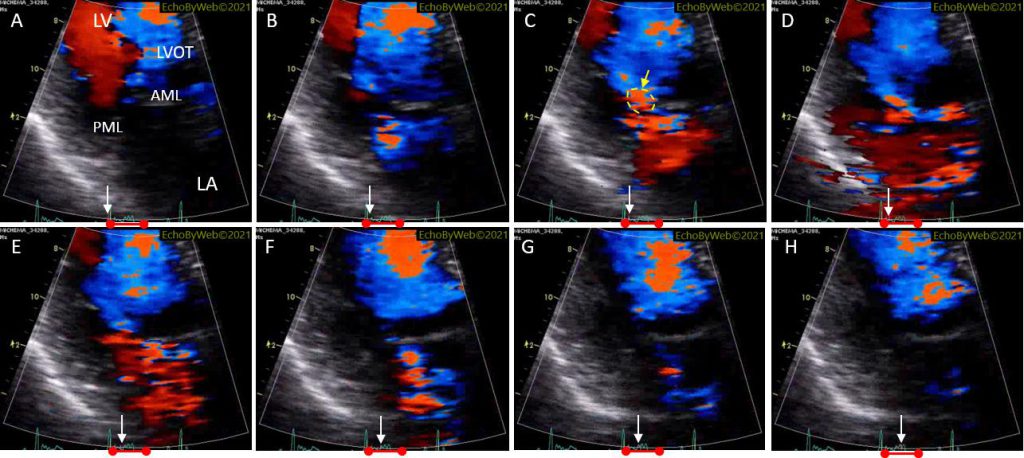
This is confirmed by a frame-by-frame analysis of color Doppler imaging in the 3-chamber view (Figure 14): the regurgitant jet appears in early systole (frame B), reaches a maximum in frames D-E, and disappears in frame G (before mid-systole). As a matter of fact, a clearly outlined area of convergence can be spotted only in frame C (yellow arrow). Finally, the continuous wave Doppler tracing of the regurgitation (shows the fading away of the signal beginning at mid-systole (Figure 12).
In conclusion, we can diagnose with certainty a secondary early systolic mitral regurgitation of grade 2 (mild). At a 7-year echocardiographic follow-up, all parameters remained unchanged, as additional confirmation of the diagnosis. The left atrial moderate dilatation was probably secondary to the combination of chronic ischemic heart disease and mild mitral regurgitation (not to mention the previous aortic valve disease).
Conclusive considerations
- Early or late systolic mitral regurgitation (not holo-systolic) is usually mild (I would also like to add: not severe by definition)
- Evaluation of Qualitative/Quantitative mitral regurgitation must be multiparametric
- It is imperative to create a personal experience for both Qualitative and Quantitative parameters