[Page 5]
Based on the echocardiographic findings a diagnosis of effusive-constrictive chronic pericarditis was made
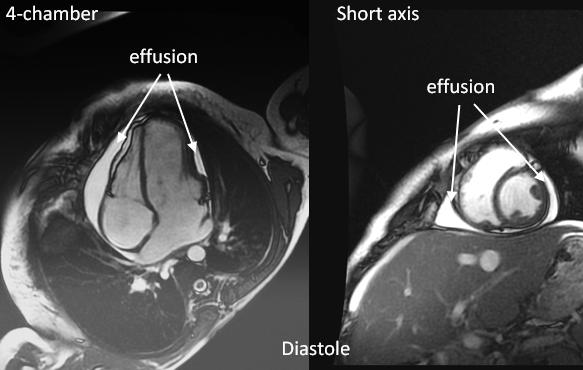
A CMRI confirmed the pericardial effusion and the typical dynamics of the interventricular septum of pericardial constriction. A CT scan showed both nodular and laminated calcifications in the AV groove and inferior pericardium, moderate pericardial effusion, mild ascites and pulmonary congestion.
A surgical pericardiectomy was proposed to the patient by the Heart Team.
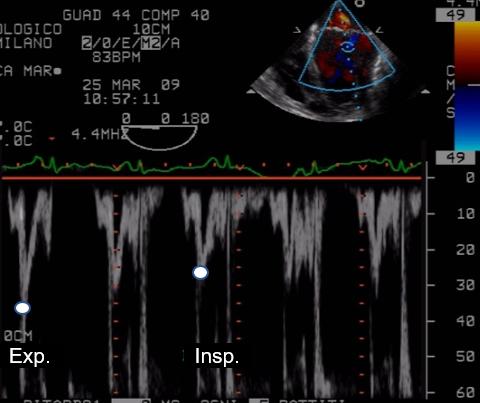
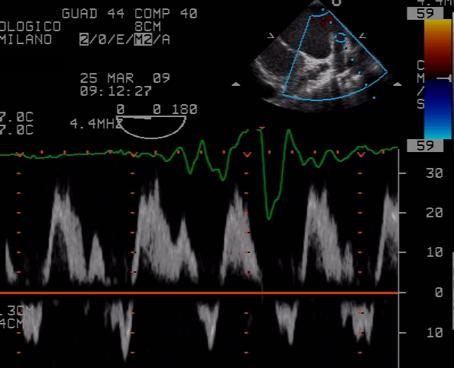
The pre-CPB transesophageal (TE) exam (Figs, 22-23) shows mild LV systolic dysfunction, moderate RV systolic dysfunction and no significant respiratory motion of the interventricular septum. The inferior pericardium is thickened (Fig 23). Transmitral (Fig. 24) and pulmonary venous flow (Fig 25) velocities show less evident variations with respiration.
Central venous pressure decreased from 17 mmHg (pre-CPB), to 13 mmHg post-CPB, and 9 mmHg (in post-surgical Intensive Care Unit).