[Page 3]
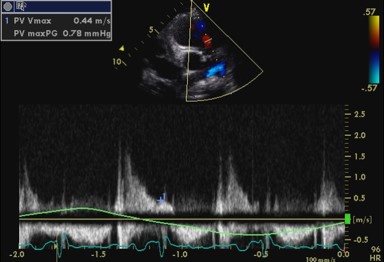
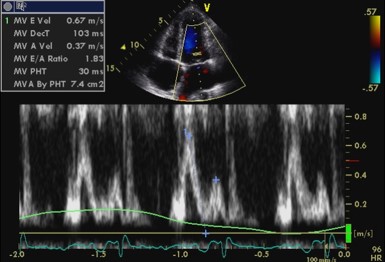
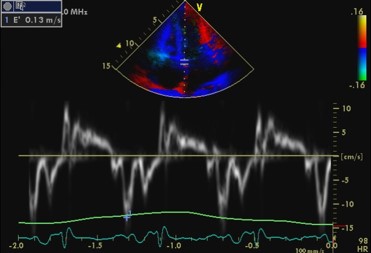
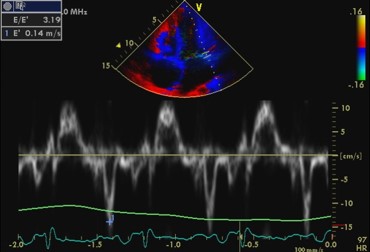
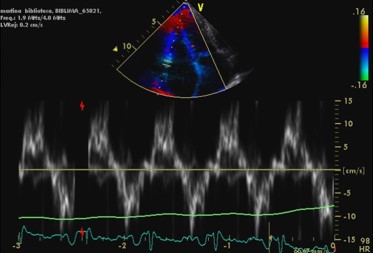
Notwithstanding the constrictive pericarditis pathophysiology, tissue Doppler imaging of the mitral annulus does not show the septal-lateral inversion of the peak velocities expected in this pathology: lateral velocities are physiologically higher than septal (Figs 14-15). The transmitral flow velocity profile is as expected in a young patient with a prevalent peak E velocity determined by normal LV relaxation, as evident from the higher septal and lateral e’ velocities (Figs 14.-15). Mean LA pressure is probably normal with E/e’ ratio= 3.2. The end-diastolic pulmonary valve gradient is low (Fig. 11). The RV tissue Doppler velocities are normal.