[Page 3]
Let’s consider this patient, admitted with a previous diagnosis of severe MR secondary to mitral valve prolapse.
At the transthoracic 2D and 3D examinations the mitral valve shows a systolic prolapse of P3. The short-axis color Doppler of the valve shows a regurgitant jet originating near the posterior commissure (not particularly evident).
He is a 65-year-old chinese male presenting with SOB since the last 3 months. He is a smoker, has non-insulin-dependent diabetes and hyperlipidemia, and normal coronary arteries. Heart rate= 80 bpm. The echocardiogram shows: normal LV end-diastolic volume= 61 ml/m2 and EF (74%), no MAD, severe LA dilatation (biplane, 71 ml/m2), mitral peak E wave= 114 cm/2, E/e’= 14, increased estimated LV filling pressures (see our online Calculator for the estimation of LV filling pressures) (Figure 8), normal pulmonary systolic pressure= 33 mmHg, and normal right ventricular dimensions and systolic function.
In this specific situation, the 2016 ASE-EACVI Diastolic Function Recommendations probably overestimate filling pressures and diastolic dysfunction class because of the increased E wave secondary to increased transmitral stroke volume (this is one of the several limitations of the current Recommendations).
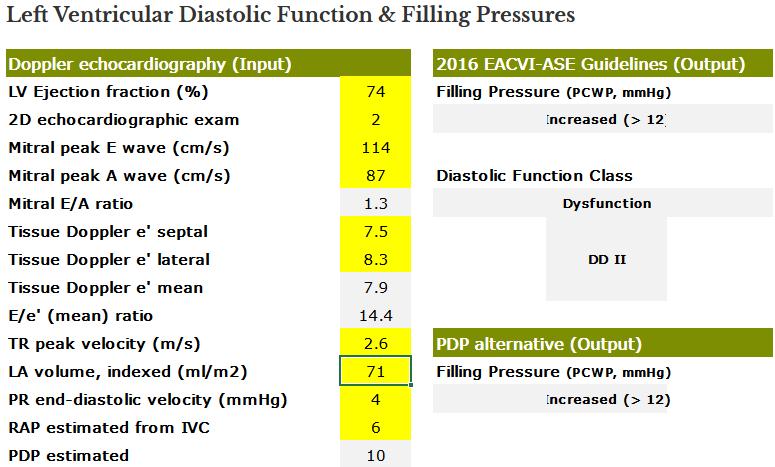
Results of the online Calculator for the estimation of LV Filling Pressures and Diastolic Function in our patient (Figure 8, right panel).
The ASE-EACVI algorithm suggests Increased LV filling pressures (> 12 mmHg) and Class II Diastolic Dysfunction. The recently published PDP algorithm equally suggests increased filling pressures (a result of increased estimated Pulmonary Diastolic Pressure + increased tricuspid regurgitation velocity + dilated LA).