[Page 5]
Transthoracic quantification of aortic regurgitation:
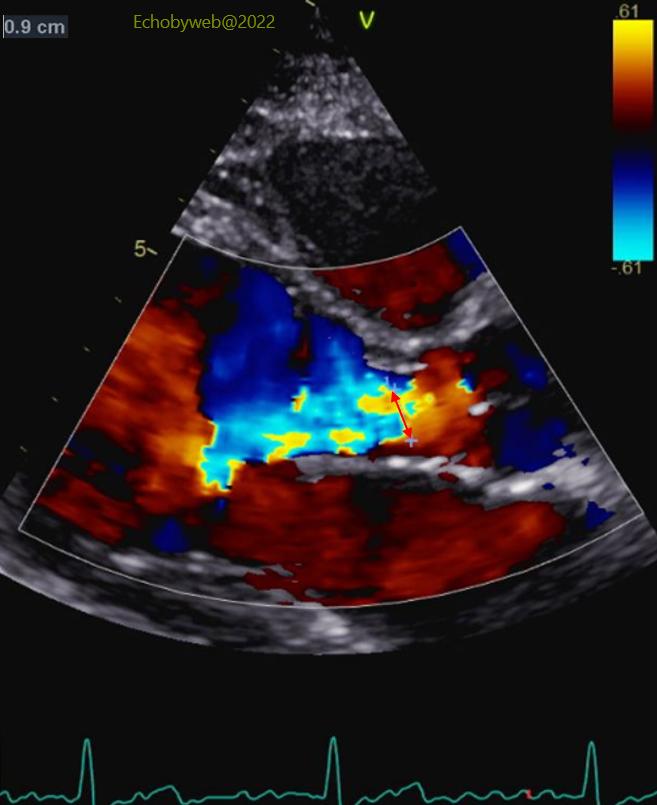
1. There was a relatively large width of the jet (9 mm) in the LV outflow tract (9 mm) with a jet/LVOT ratio of 42% (= moderate regurgitation) (Figure 15, red double-headed arrow).
2. The LV outflow tract velocity-time integral was increased to 28 cm (not shown) (compatible with mild/modertate, not with severe).
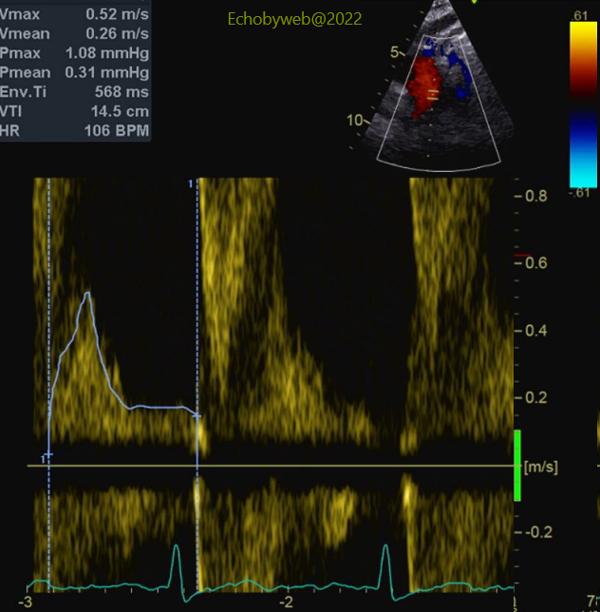
3. The aortic diastolic backflow velocity-time integral= 14.7 cm (Figure 17) did not confirm severe regurgitation. I personally prefer to measure the velocity-time integral (cutoff for severe regurgitation: > 17 cm), rather than the end-diastolic velocity.
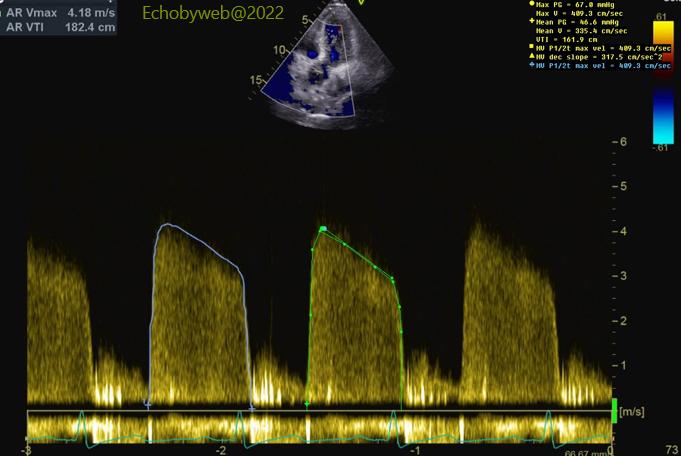
4. The density of the continuous-wave diastolic velocity-time integral of the aortic regurgitation was intermediate; the diastolic slope was 320 cm/s (Figure 16).
5. The PISA evaluation showed: Regurgitant volume= 38 ml; EROA= 0.23 cm2.
6. The Doppler stroke volume method showed: Regurgitant volume= 18 ml; regurgitant fraction: 19%; EROA= 0.11 cm2. This method probably underestimated the grade of regurgitation.
7. Finally, as mentioned above, the volumes of the LV were normal and the end-systolic diameter= 35 mm. Of note, the GE AFI strain examination did not show any subtle myocardial dysfunction.
The decision was made at the Heart Team discussion to discharge the patient in medical therapy with enalapril for optimal blood pressure control, having judged the severity of aortic regurgitation as moderate, and the status of the patient as too early for aortic valve replacement surgery. A follow-up echocardiographic study was suggested (at 3-6 months) to evaluate any progression of LV dimensions.
The apparent severe grade of regurgitation seen at the transesophageal examination was probably related to uncontrolled blood pressure.