[Page 2]
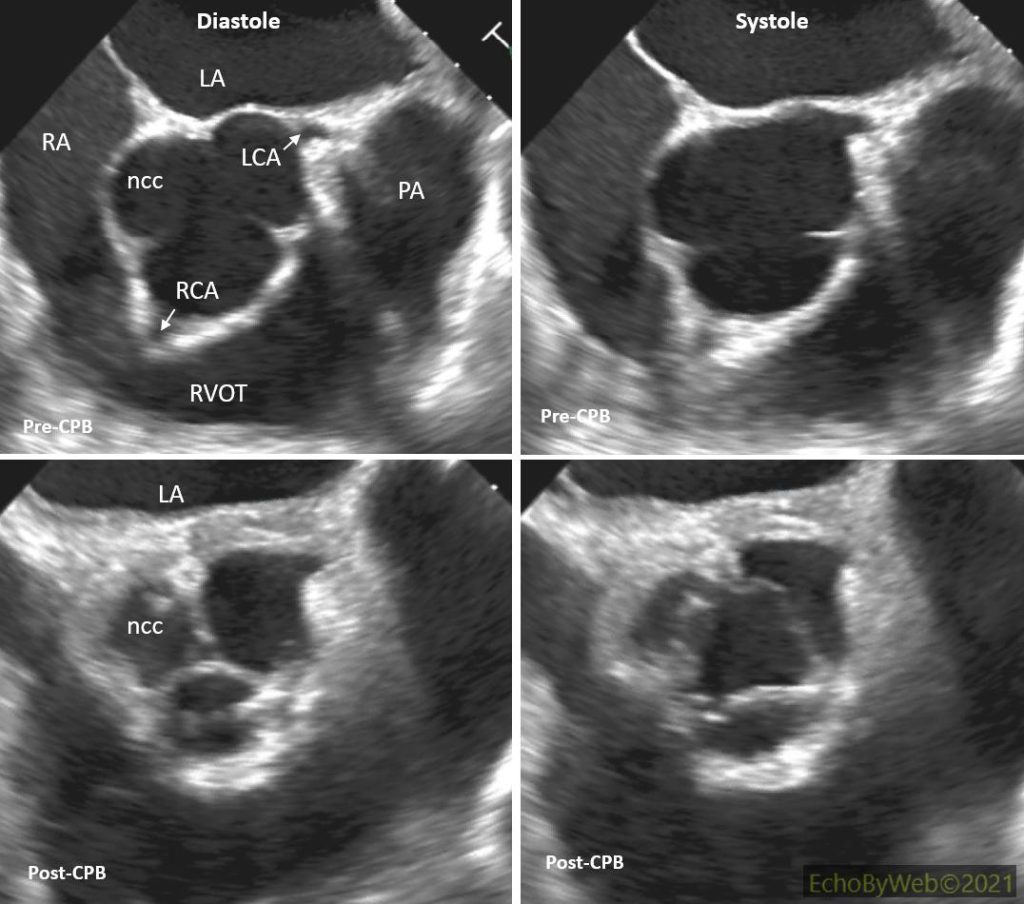
Figures 5-7. TE exam pre- and post-CPB. In the post-CPB images the AV neo-cusps are clearly seen with opening and closure dynamics similar to those of the native cusps. Notice the perfect apposition in diastole between the cusp margins, and the thickened commissures (surgical sutures).
LA: left atrium; LCA: left coronary ostium; ncc: posterior non-coronary cusp; RA: right atrium; RCA: right coronary ostium.
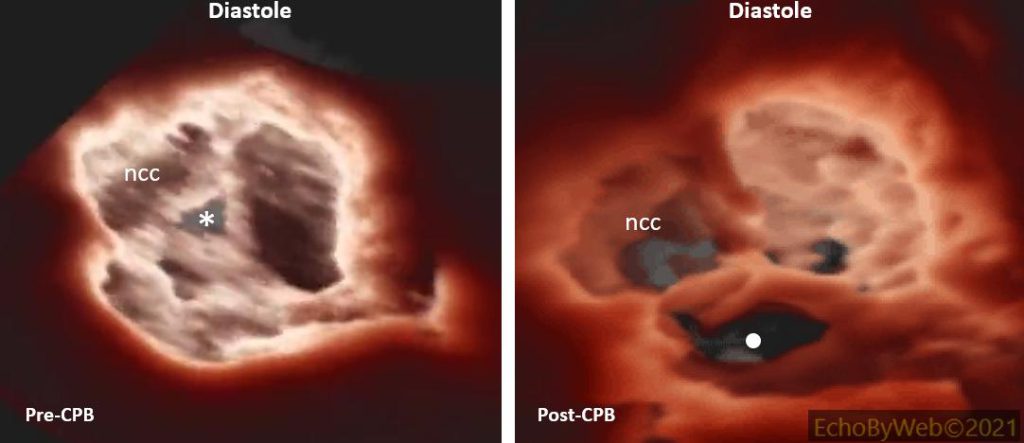
Figures 8-10. 3D imaging (with transillumination, Philips Epic7c unit) of the AV in short axis, as viewed from the aortic root. Note the incomplete central apposition of the cusps of the native valve (asterisk), causing severe AR, (Image 1). The dot in the post-CPB image points to tissue defect artifact: gain was kept low to optimize imaging of the perfect diastolic apposition of the neo-cusps.