[Page 3]
Pericardial adhesions and pericardial fat.
Echocardiographic examples: differences between pericardial fat (Figure 11) and pericardial adhesions following effusion and organization (after CABG) (Figure 12).
Pericardial fat. In this case, a “speckled” structure is seen within the pericardial space, with the pericardium and epicardium freely sliding over the fat. This patient was admitted to the ER for shortness of breath and palpitations. There is severe prolongation of LV relaxation (markedly reduced tissue Doppler e’), moderate RV hypertrophy with normal systolic function, mild aortic stenosis (valve planimetry and continuity equation), ischemic heart disease with moderate reduction of EF, and normal LV filling pressures. There is abundant pericardial fat lateral to the right heart chambers.
Pericardial adhesions. In this case, “tugging” of the pericardium may be seen during myocardial contraction: the epicardium drags the pericardium during systole (secondary to adhesions between epicardium and pericardium), whereas in normal physiology (no adhesions) the epicardium slides beneath the pericardium. In this patient, the adhesions follow a recent CABG, without signs of pericardial constriction.
Pericardial Effusion
M-mode and 2D diagnosis of mild (Figures 11-12) and severe effusion (Figure 13-14).
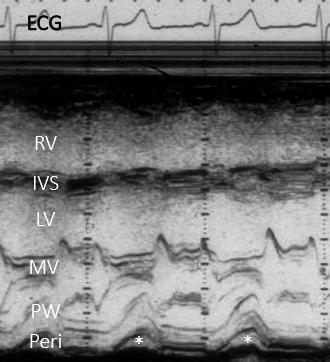
Example of mild (Figures 11 and 12) effusion. In this patient M-mode shows effusion only in systole (asterisks), whereas 2D imaging shows effusion visible along all the cardiac cycle.
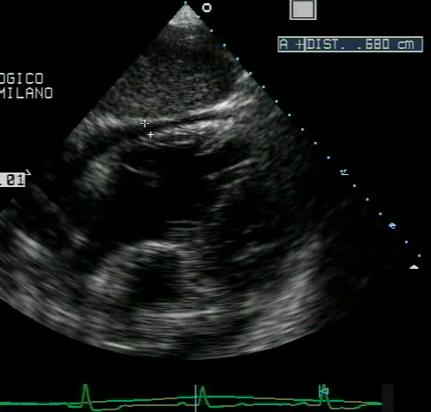
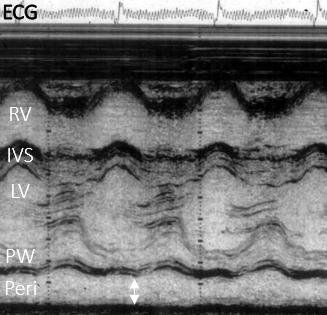
Example of severe (Figure 13 and 14) effusion. The quantification of the effusion should be performed at end-diastole (Figure 13, white double arrow). The 2D subcostal imaging describes well the severe diffuse effusion.
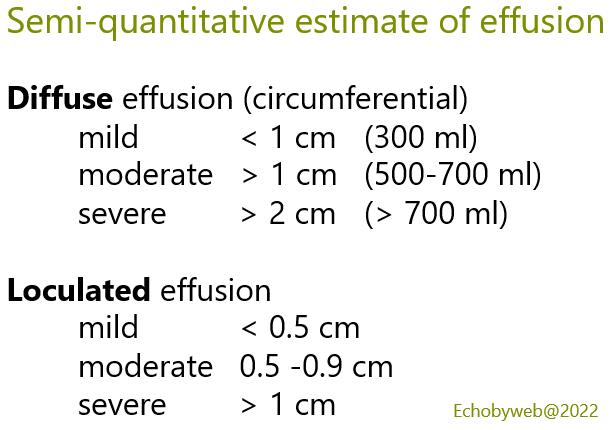
Estimation of the severity of diffuse effusion.
Modified from: D’Cruz IA et al. A new cross-sectional echocardiographic method for estimating the volume of large pericardial effusion. Br Heart J 1991;66:448.
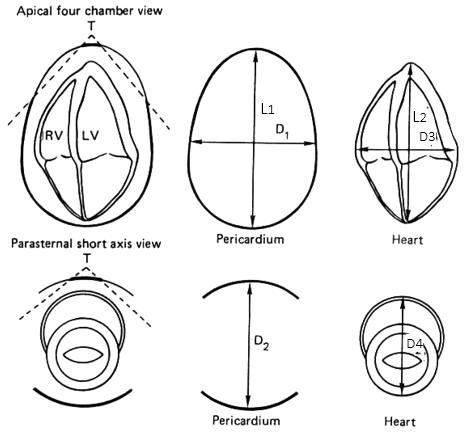
Figure 17. Measurement of diffuse pericardial effusion.
Pericardial measurement (pericardium, outer shell): measure the maximal long axis dimension (L1) and maximal transverse dimension (D1) in the apical 4-chamber view, and the maximal anteroposterior dimension (D2) in the parasternal long or short axis view at the mitral leaflet level.
Epicardial measurement (heart, inner shell): measure the maximal long axis dimension (L2, from the tip of ventricular apex to the cephalad border of atria at the junction of right and left atrium in the apical 4-chamber view) and the maximal transverse dimensions (D3) in the apical 4-chamber view (at the level of the mitral and tricuspid leaflets, 1 to 3 cm on the ventricular side of the atrioventricular valve annuli) and the maximal anteroposterior dimension in the parasternal long or short axis view (D4) at the mitral leaflet level.
The 2 pericardial and epicardial volumes are calculated by applying the formula for the volume of a prolate ellipse:
π x 4/3 x L/2 x D1/2 x D2/2, where L is the major axis and D1 and D2 the 2 minor axes. The pericardial effusion volume is calculated as the difference between the 2 volumes= pericardial – epicardial. Use the Online Calculator to estimate Pericardial Effusion Volume.
Semi-quantitaive estimation of pericardial effusion.